
 Welcome, Guest. Please
Welcome, Guest. Please  May 04, 2024, 11:27:26 am
May 04, 2024, 11:27:26 am
1
Do I Have HIV? / Re: ARS symptoms next day ?
« Last post by Jim Allen on Today at 11:21:05 am »It's not HIV related
|
||||||

|
|
|
Welcome to the POZ Community Forums, a round-the-clock discussion area for people with HIV/AIDS, their friends/family/caregivers, and others concerned about HIV/AIDS. Click on the links below to browse our various forums; scroll down for a glance at the most recent posts; or join in the conversation yourself by registering on the left side of this page. Privacy Warning: Please realize that these forums are open to all, and are fully searchable via Google and other search engines. If you are HIV positive and disclose this in our forums, then it is almost the same thing as telling the whole world (or at least the World Wide Web). If this concerns you, then do not use a username or avatar that are self-identifying in any way. We do not allow the deletion of anything you post in these forums, so think before you post.
To change forums navigation language settings, click here (members only), Register now
Para cambiar sus preferencias de los foros en español, haz clic
aquí (sólo miembros), Regístrate ahora |
 Recent Posts
Recent Posts
You cant get HIV from getting a blow job
Interesting, but this kind of contradicts the whole widespread use of antibiotics unnecessarily will create resistance argument.
The second objection was to do with antimicrobial resistance which is, BREACH says, a huge concern in STI and other bacteria, with some studies showing an increase in antimicrobial resistance.
The conclude: Considering that the number needed to treat to avoid a symptomatic infection with gonorrhoea or chlamydia is probably very high, the considerable potential to select resistance in STIs and other bacterial species and the possibility of disrupting the microbiome, it is considered that the potential individual benefits of doxyPEP are outweighed by the risks in men who have sex with men.
They recommend that, if doxyPEP is to be prescribed, is should only be done as part of a research study.
HIV clinicians have issued a note of caution regarding long-acting injectable cabotegravir and rilpivirine in a recent commentary in AIDS. Dr Diego Ripamonti of the Papa Giovanni XXIII hospital in Bergamo and colleagues from the universities of Milan and Siena highlight that people with long treatment histories in particular may not be good candidates for the treatment, due to the substantial risk of developing resistance to the drugs should the treatment fail.
In clinical trials, injectable cabotegravir and rilpivirine was found to be similarly effective to daily pills in suppressing HIV to undetectable levels.
However, in the small minority of participants for whom injectable treatment didnt work (around 1% (26/2313) of participants in the five main clinical trials), there was a high rate of emergent resistance to integrase inhibitors. Having resistance to these drug types is a big problem for patients as it greatly limits the types of HIV treatment that will effectively suppress their HIV.
The authors point out that while taking pills 8085% of the time is enough to avoid treatment failure with most modern HIV treatments, some of those who developed drug resistance to injectable cabotegravir and rilpivirine in the trials had perfect adherence.
They also highlight that the level of emergent resistance in injectable cabotegravir and rilpivirine trials is higher than any other simplified drug regimen, even including dolutegravir monotherapy a drug regimen which has been criticised by many experts and is not recommended for use.
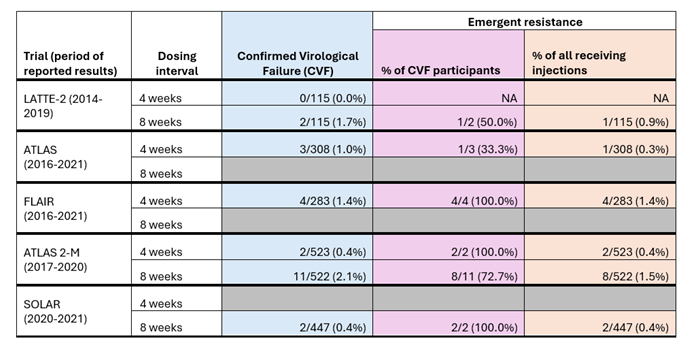
The table includes data on emergent resistance this means that resistance to integrase inhibitors (like cabotegravir) or NNRTIs (like rilpivirine) was not detected in blood samples taken before the participants started injectable treatment and was detected in blood samples after the participants started injectable treatment.
The table shows that the number of people who experienced confirmed virological failure (column in blue) was very small, Of those with confirmed virological failure (column in purple), the rates of emergent resistance were high, ranging from 33.3%-100%.
Consequently, the authors make the following recommendations:
- Factors that put people at risk of developing drug resistance should be thoroughly investigated before prescribing injectable cabotegravir and rilpivirine. In particular, clinicians should aim to use DNA resistance testing to detect archived mutations, although this test is not always available.
- Doctors should be cautious when prescribing long-acting injectable cabotegravir and rilpivirine to patients with long and/or complex treatment histories. In addition, people with low CD4 cell counts or previous experience of AIDS were excluded from clinical trials, and might also be at risk of treatment failure.
- Before switching a patient to injectable cabotegravir and rilpivirine, clinicians should proactively identify their remaining treatment options should they experience treatment failure and develop resistance to both drugs.
As appealing as this long-acting option may appear, both clinicians and people with HIV should be aware of the associated risks, carefully weighing all baseline factors and planning the appropriate exit strategy in the event of failure, conclude Dr Ripamonti and colleagues.
Terms of Membership for these forums

|
|
© 2024 Smart + Strong. All Rights Reserved. terms of use and your privacy
Smart + Strong® is a registered trademark of CDM Publishing, LLC.